Tibial Shaft Fracture
What is a Tibial Shaft Fracture?
A tibial shaft fracture is a break of the larger lower leg bone below the knee joint. This occurs along the long portion of the bone between the knee and ankle joints. These fractures usually result from high energy injuries such as car accidents in younger patients and most often from falls in the elderly patient. The tibia can be broken into many pieces or just crack slightly depending on the quality of bone and the type of injury.
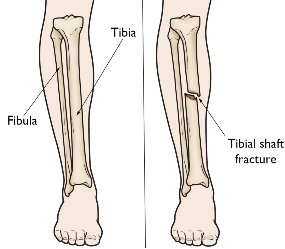
Illustration of tibial shaft. Reproduced with permission from OrthoInfo. © American Academy of Orthopaedic
Surgeons. https://orthoinfo.org/
What does the Tibia do?
The tibia is the most important lower leg bone because it supports your body weight as you walk, run and jump. It is a vital part of the knee and ankle joints. It must heal straight to allow these joints to work well. Many important muscles also attach to this bone, which help the thigh, leg and foot muscles work properly.
Diagnosis and Examination
Physical examination is important in the evaluation of these injuries. Important nerves and blood vessels run next to this bone and can be injured when it break. The doctor will look for any open wounds over the injury as these usually require surgery. Often, the bone tries to poke out of the skin or “tent.” If this is not corrected, the skin can die or the bone can eventually cut the skin.
Patients with a broken tibia are at risk for a serious condition called compartment syndrome. This occurs when the pressure in the leg gets too high for blood and oxygen to circulate. Eventually the muscle will die if this goes untreated. Signs of this syndrome are severe pain with stretch of the big toe, loss of sensation in the foot or pain out of proportion to the injury itself. This is a surgical emergency. This test may feel like your doctor is trying to torture you when you already have a broken bone but this exam is very important.
X-rays are used to evaluate the location and severity of the broken bone. This helps doctors and patients make an informed decision on treatment. Often two or more x-rays are taken to show the injury pattern. A CT (Computed Tomography) scan is often ordered if the break extends into the knee or ankle joint.

Tibial Shaft Fracture X-Ray
Non-Surgical Treatment for Tibial Shaft Fractures
Although most broken tibias in adults are treated with surgery, some fracture patterns and types do not need surgery for the bone to heal. In children, many types of tibial shaft fractures can be treated with casts. Nonsurgical treatment is also recommended for adults with poor overall health, fragile or chronically infected skin, less active patients and in fractures with near perfect alignment.
If non-operative care is chosen, regular follow-up care for a physical exam and x-rays is important to ensure that the fracture stays in good position and heals appropriately. Cutting down or quitting smoking and tight blood sugar control if you are a diabetic is important for the healing process. One fall or continued lack of compliance with casting, bracing or early walking against medical advice can cause bones to move and result in the need for surgery.
Depending on health and injury pattern this bone can take 3-4 months to heal without surgery. In the initial few weeks, fractures treated without surgery tend to be painful or uncomfortable until the healing process matures over a few weeks. Physical therapy for knee and ankle range of motion is started around 6 weeks once bone has healed enough to prevent displacement with motion.
Surgical Treatment for Tibial Shaft Fractures
Surgeons may recommend an operation to fix the broken tibia if the pieces are displaced, if the bone sticks out of the skin, if skin is at risk for dying or if the bone is unstable due to the fracture type. The tibia can be fixed with metal plates and screws placed through large incisions or intramedullary nails which use small incisions. The type of fracture usually dictates what type of metal and surgery needs to be done. The most common treatment for tibial shaft fractures is an intramedullary nail because it can be done with percutaneous small incisions, has a very high healing rate and patients can often bear weight and walk on this right after surgery. Metal plates and screws are used in children who need surgery to avoid the growth plates and in adults with fractures close to or involving the knee or ankle joints. Surgery usually takes 1 to 2 hours. Most patients are admitted overnight after tibial nailing procedures to watch for any breathing problems or development of compartment syndrome.
In cases where there is severe injury to the muscles, nerves or arteries or there is significant contamination with dirt, rocks or grass from the injury, some patient require external fixation prior to definitive surgical treatment. This is an operation where metal pins are placed into the bone through small cuts and connected to bars to give some stability to the bone. After secondary operations to clean the wound or recovery of skin injuries, the external fixator can be removed and an intramedullary nail or plates and screws can be placed.
Ideally, surgeons like to perform this surgery acutely or at most within 1-2 weeks of injury. Thus, patients have time to seek a second opinion regarding treatment if more information or additional surgeon input is desired.
It is important to choose your surgeon wisely. Extensive surgical experience can be helpful in achieving a good result and avoiding complications. Collectively, ROC orthopedic surgeons have performed more tibia operations than any practice in Northern Nevada and take pride in outstanding surgical results.
After surgery, patients are often placed in a splint or walking boot and often can bear weight immediately. If the smaller ankle bone (the fibula) is badly broken, weight bearing may be delayed. Gentle motion is begun early to prevent stiffness. Gradually this motion is increased and physical therapy is begun around 6 weeks after surgery if the patient has residual knee or ankle stiffness.
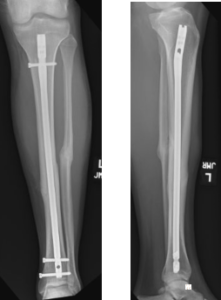
Postoperative x-ray of tibial shaft fracture.
Surgical Complications
Complications can occur with any surgery, no matter how small. There is always a risk of infection. The risk is much bigger for larger and more contaminated traumatic wounds. A dose of antibiotics given prior to surgery helps to make this risk as small as possible.
There is always a risk of injury to blood vessels or nerves. This is reduced by having an experienced surgeon involved in your care. As stated above, compartment syndrome can occur from the injury and evolve during surgery. This requires additional surgery to release the pressure on the muscles. Noncompliance with weight bearing restrictions, too much motion or falls can result in the metal ripping out of the bone or the fracture separating. It is always possible that the bone may not heal and additional surgery will be required. This is usually associated with patient noncompliance, diabetes, or use of nicotine like smoking and chewing tobacco.
Outcomes
Most people with tibial shaft fractures do very well and return to prior activities and function. By six weeks, patients are extremely comfortable and usually are released to full activities such as manual labor, skiing and motocross by four months. Aggressive return to activity too early can result in re-fracture, hardware breakage or nonunion.